







ESSENTIAL READ: Facts and data without the sensationalism and political agenda at last!
If you only read one article about COVID-19, this is the one:
Dr. Zoë Harcombe
zoeharcombe.com
Fri, 20 Mar 2020 11:12 UTC

I’ve been writing a Monday note since 2009. The topic has usually been inspired by what’s in the news from a diet or health perspective. Whether the EAT Lancet diet being launched on the world, or the latest epidemiological paper to come out of Harvard – the topic that has made the headlines has been the one most likely to be featured.
This week there is only one health news story and it’s the same story worldwide – Coronavirus. I’ve been reticent to write about it, as the situation is uncertain and continuous, and this note will date faster than any I have written. (Hence why it’s coming out early – to be as current as possible). But it is the topic of most interest and so l will approach this topic as I would any other – What are the facts? What does the data tell us? Where best to find more information? I found the note very interesting to research and I hope you find it interesting to read…
What is Coronavirus? (Ref 1)
Coronaviruses (CoV) are a family of viruses that are called “zoonotic”, meaning that they are transmitted between animals and people. The word Corona in Latin means crown or garland. They are called coronaviruses because each virus particle looks like it is surrounded by a crown/garland when viewed under a microscope. There are four main sub-groupings of coronaviruses, known as alpha, beta, gamma, and delta.
Human coronaviruses were first identified in the mid-1960s. The seven coronaviruses that can infect people are split into ones that people commonly get around the world, but that have mild symptoms:
- 229E (alpha coronavirus)
- NL63 (alpha coronavirus)
- OC43 (beta coronavirus)
- HKU1 (beta coronavirus)
and three others, which have proved more serious:
- MERS-CoV (the beta coronavirus that causes Middle East Respiratory Syndrome, or MERS)
- SARS-CoV (the beta coronavirus that causes severe acute respiratory syndrome, or SARS)
- SARS-CoV-2 (the novel coronavirus that causes coronavirus disease 2019, or COVID-19)
When we are talking about ‘the coronavirus’ today, we are talking about COVID-19. This is a new coronavirus, which has not previously been identified in humans. We are dealing with something quite unknown with COVID-19, but we can learn some lessons from MERS-CoV and SARS-CoV. A paper published in theEuropean Journal of Immunologyon February 27th called “COVID-19: Lessons from SARS and MERS” is a valuable resource for anyone interested in understanding how the viruses are similar and different (Ref 2).
SARS-CoV originated in China in 2002 and ‘burned out’ in the summer of 2003 with the high temperature and humidity of the summer months helping to kill the virus. There have been no known cases of SARS anywhere in the world since 2004 (Ref 3). MERS-CoV was first identified in the Middle East in 2012. There is evidence that it is transmitted from camels, although transmission to humans is rare. There have been just five cases of MERS in the UK since 2012 (Ref 4). Neither virus has a vaccine, but it is likely that interest in developing one fizzled out alongside the numbers of people affected.
How did COVID-19 start?
The South Morning China Post reported that a 55-year old individual from Hubei province in China may have been the first person to have contracted COVID-19 on November 17th, 2019 (Ref 5). An academic paper published in The Lancet on January 24th 2020 reported on a cluster of pneumonia cases in Wuhan, China, caused by a novel coronavirus, which had been named 2019-nCoV (Ref 6). The article had undertaken a search to see if any other papers had been published about this new virus. It reported “No published work about the human infection caused by the 2019 novel coronavirus (2019-nCoV) could be identified.” This, therefore, appears to be the first academic paper about the virus.
This seminal Lancet paper reported that, by January 2nd, 2020, 41 patients had been confirmed to have what they called 2019-n-CoV (now called COVID-19). Of these 41 patients, 27 had had exposure to Huanan seafood market. The first patient of the 41 – identified on December 1st, 2019 – had not been to that seafood market. The common symptoms were fever (40 out of 41 patients), cough (31 out of 41) and fatigue (18 out of 41).
This paper reported that the Middle East Respiratory Syndrome coronavirus (MERS-CoV) and the Severe Acute Respiratory Syndrome coronavirus (SARS-CoV) had resulted in approximately 10,000 cases between the 2 viruses in the past 2 decades. The mortality rates were reported as 10% for SARS-CoV (Ref 7) and 37% for MERS-CoV (Ref 8), so we should be thankful that the case numbers were relatively small.
The first two cases of COVID-19 were reported in the US on January 14th, 2020 (Ref 9). The first case was reported in Australia on January 25th (Ref 10). The first two cases were reported in Italy on January 30th (Ref 11). The first two cases were reported in England on January 31st, 2020 (Ref 12).
What are the symptoms?
Common symptoms of having a coronavirus included fever, cough, shortness of breath and breathing difficulty. A British politician, Nadine Dorries, and a General Practitioner (Family Doctor) and former chair of the Royal College of General Practitioners, Clare Gerada, have recently recovered from COVID-19 in the UK and they have shared their experiences. Nadine is 62 years old and Clare is 60; both are fit and healthy women.
Nadine said that she started feeling “slightly unwell” and soon was experiencing fever, night sweats (to the point of soaking the sheets), sore eyes, a persistent cough (which was dry and unproductive) and every muscle and bone ached. She has been left with a residual cough and the feeling that her lungs have not yet fully recovered (Ref 13).
Clare returned from a conference in New York feeling like she had jet lag. This was soon followed by a temperature of above 102°F (38.9°C) and Clare realised that she had the virus. She spent the next five days in bed with flu-like symptoms – fever, dry cough, sore throat, bad headache, muscular chest pain from coughing (Ref 14). Clare reported a marked loss of appetite and I have seen this reiterated in other accounts from people who have recovered from the virus.
Chris Gough, an Anaesthetist, has had over half a million likes and retweets of his twitter thread detailing what he went through when he got the virus (Ref 15). I found this thread worth bookmarking because Chris detailed what happened on day 1, day 2 etc. Response to the virus will be individual, but this may be useful to look at if you develop symptoms.
The three key symptoms of COVID-19 are reported as fever, cough and shortness of breath (Ref 16). We understand that these can occur between 2-14 days after exposure, based on what has been observed with the MERS Co-V viruses. Most people will feel like they’ve got a particularly nasty dose of flu – for approximately seven days – and then recover. The minority of people – especially those with existing heart disease, respiratory disease, diabetes, hypertension, and/or cancer – develop more serious breathing difficulties and those are the ones advised to contact the emergency services.
Where can I get the latest information and data?
Many more academic papers have been published since that Lancet article. The academic database, PubMed, can be searched for “COVID-19” and “humans.” I did this and there were 99 results at the time of researching for this note (Ref 17). Papers range from individual case studies… to doctor experiences being shared to help other medics… to review articles about the virus particularly, or epidemics/pandemics generally. There’s even a paper about anti-Chinese sentiment during the outbreak.
The official information sites are the World Health Organization (WHO) (Ref 18), the CDC (US) (Ref 19), the NHS (UK) (Ref 20) and the Department of Health in Australia (Ref 21). Search engine companies have been working to ensure that the official advice is at the top of any searches that you do in your country.
The best real time data seems to be coming from Worldometers (Ref 22). This has more data, more up to date data and more different ‘cuts’ of the data than the WHO “situation” page (Ref 23). Worldometers is run by an international and independent team of developers, researchers, and volunteers. The team’s aim is “to make world statistics available in a thought-provoking and time relevant format to a wide audience around the world.” Their Coronavirus section provides the latest numbers of cases, deaths and recoveries per country (Ref 24). The data are also provided for men vs women, younger vs older people and people with different pre-existing conditions vs without.
What are the numbers?
The single most important thing to say about the numbers is that they’re wrong. There are two particular ways in which they are wrong, and we need to be aware of these, so that we don’t scare people unnecessarily:
1) Deaths will be the most accurate number, as official records are kept on deaths. The number of cases is the inaccurate number. We have not been testing anywhere near enough people and therefore the number of cases will be substantially underestimated.
2) The people most likely to have been tested are those who have symptoms of the virus. This is a form of confirmation bias. It will pick up more cases than there are in the general population, but it will miss the mild cases among the general population and thus again underestimate the number of cases and overestimate the severity of cases.
Both (1) and (2) will have the effect of making the death rate (deaths/number of cases) look worse than it really is (Ref 25).
The numbers are also changing every few minutes, so the following precise numbers will be out of date by the time you see them. They do, however, give a guide to the countries and types of people facing the greatest challenges and so are useful for trends and knowledge.
When I started writing this note, on 17th March, there were 189,000 cases worldwide, over 80,000 of which were recorded in China (42%). China did have all the cases (100%) in the beginning of this virus. China’s proportion of the cases is falling by the day, as case numbers rise in other countries. On the 17th March, Italy had the second highest number of cases in the world, followed by Iran, then Spain and then South Korea.
I updated the numbers at 7am on Friday 20th March and South Korea had fallen out of the top five. Italy has just overtaken China for the number of deaths. I’ve kept S Korea in the following table, as its testing numbers are interesting. China’s proportion of cases has dropped to 33% in 3 days.
The table below is a snapshot of the top five countries, plus S Korea. This illustrates available data. You can get the latest numbers from the Worldometers site and/or for your own country, as desired.
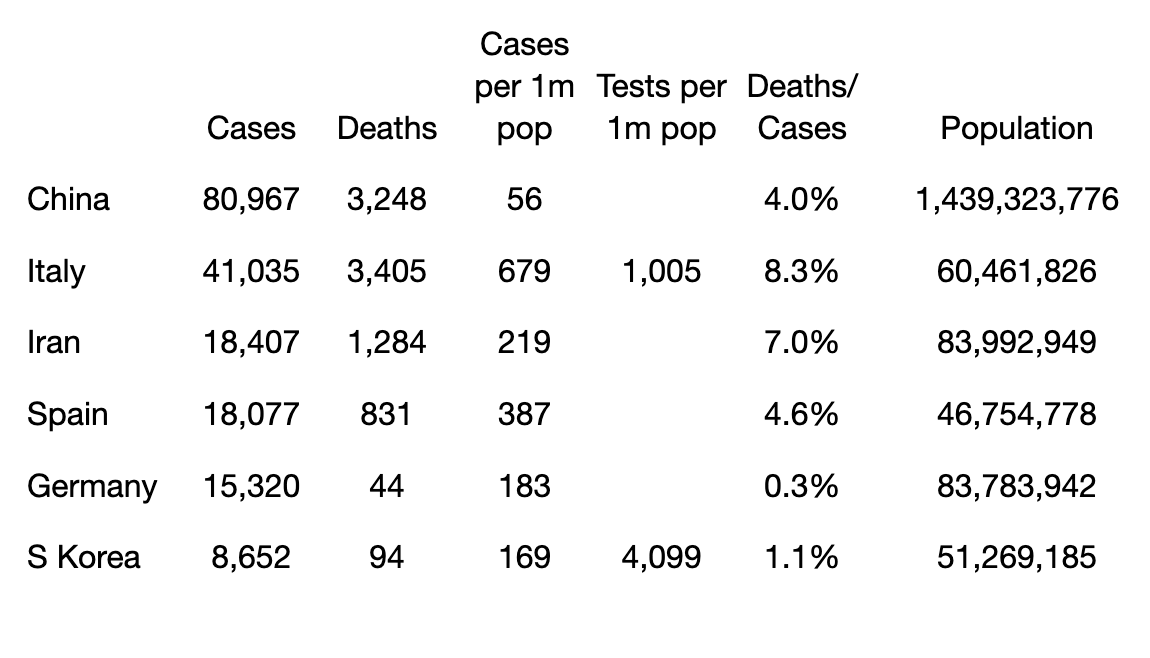
The table extracts data for: cases, deaths, cases per 1 million people in that country, tests per 1 million people (these data are not available for most countries and the two numbers above were from March 9th, 2020) and the population of each country. I have also calculated deaths per number of cases. This is NOT an accurate picture of the death rate, as I started to explain above and continue here…
As you can see from the table, testing has been very low, and we don’t even know the testing rate in most countries. The key message from the WHO conference on March 16th, 2020 was “test, test, test” (Ref 26). We don’t know what we’re dealing with without facts. Testing has been grossly insufficient worldwide since this virus started. Don’t think, from the table above, that S Korea has a death rate of 1.1% and Italy has a death rate of 8.3%. Italy has tested a quarter of the number of people that S Korea has. It may be the case that half the Italian population has the virus, and thought they had flu, in which case the death rate would be 0.007% – you won’t be able to get your head around such a small number.
A tweet on March 13th questioned: “Can anyone explain how a virus (identified in Wuhan in Dec 2019) spread to the Canadian prime minister’s wife, one of Hollywood’s top actors & his wife, a Premier League football manager, and a British member of parliament – within 16 weeks – while bypassing the majority of us?” (Ref 27). The answer is, of course, it didn’t. Many of us have, or have had, the virus already.
The high risk groups
The data on Worldometers can be cut by sex, age and existing conditions. This is where the numbers can appear scary, but keep in mind that we are underestimating case numbers. The three messages that we get from demographics are:
1) Sex: Worldometers calculates the deaths/cases to be 2.8% for men and 1.7% for women. Smoking is a risk factor for respiratory diseases; most of the deaths have been in China (until this morning) and 52% of men smoke in China vs 2.7% of women (although women are exposed to second-hand smoke) (Ref 28). If you’re male and don’t smoke, this should reassure you. If you are a smoker of either sex, it is recommended to do whatever you can to quit now. Smoking up to the point of contracting the virus won’t help chances of recovery.
Comment: That’s the typical party line, but evidence exists that smoking is actually protective against coronavirus (and many other diseases). See: Study on Coronavirus patients in Wuhan suggests non-smokers are more likely to become infected
2) Age: Worldometers calculates the deaths/cases to be as follows per age group:

Italy is the country to mention in the age category. There are a number of different ways of calculating the age of a population. Italy has the third oldest population in the world when calculated by people over 65 per working age people (Ref 29). An article on Italy was shared by a Swedish American academic in an email thread (Ref 30). People who have died in Italy had an average age of over 80, were predominantly male (think smoking again) and had an average of 2.7 pre-existing health conditions (Ref 31).
We all have older loved ones and the numbers for older people have been the most worrying but i) keep remembering that this number is higher than the truth and ii) pre-existing conditions overlap significantly with age. Older people are more likely to have other conditions (see the next section).
3) Pre-existing conditions: Worldometers calculates the deaths/cases to be as follows per pre-existing condition:
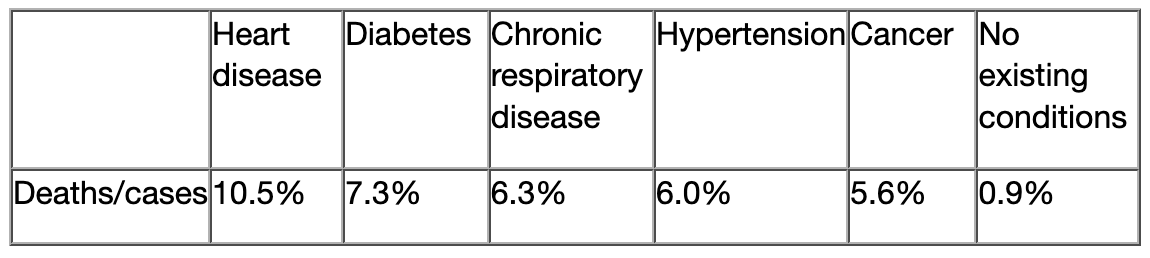
The 0.9% deaths/cases for “no existing conditions” cuts across all ages, so the reassurance for healthy older people should come from this existing condition data. The current strategy to protect older people and those with existing conditions should perhaps focus more on the latter than the former, but caution is wise for all higher risk groups when facing unknowns.
Reassuring numbers
There are enough scary numbers being shared at the moment. Here are three that reassure me:
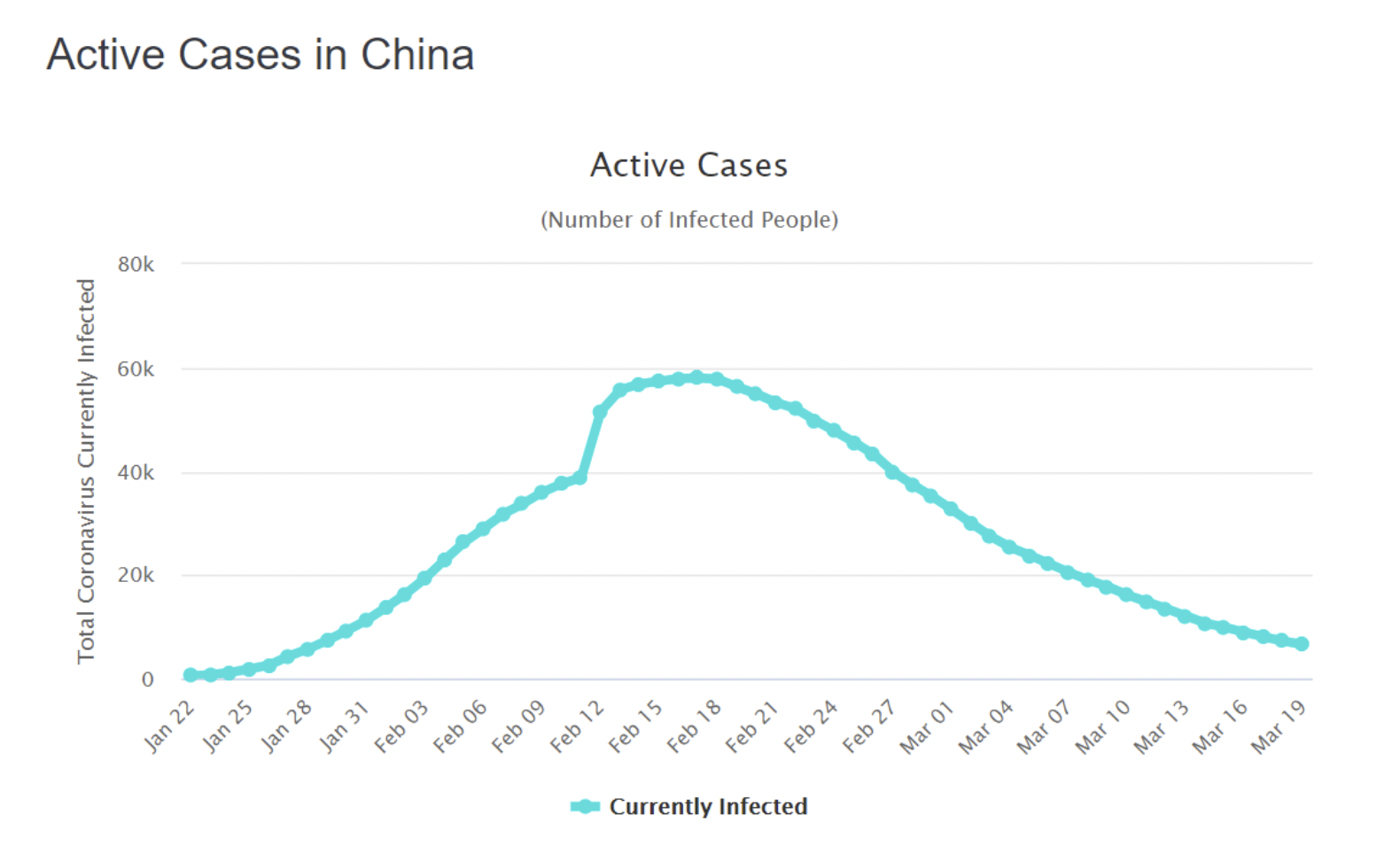
1) The number of active cases has peaked and is on the decline in the country that first experienced the virus. (This does provide support for China’s response to the virus).
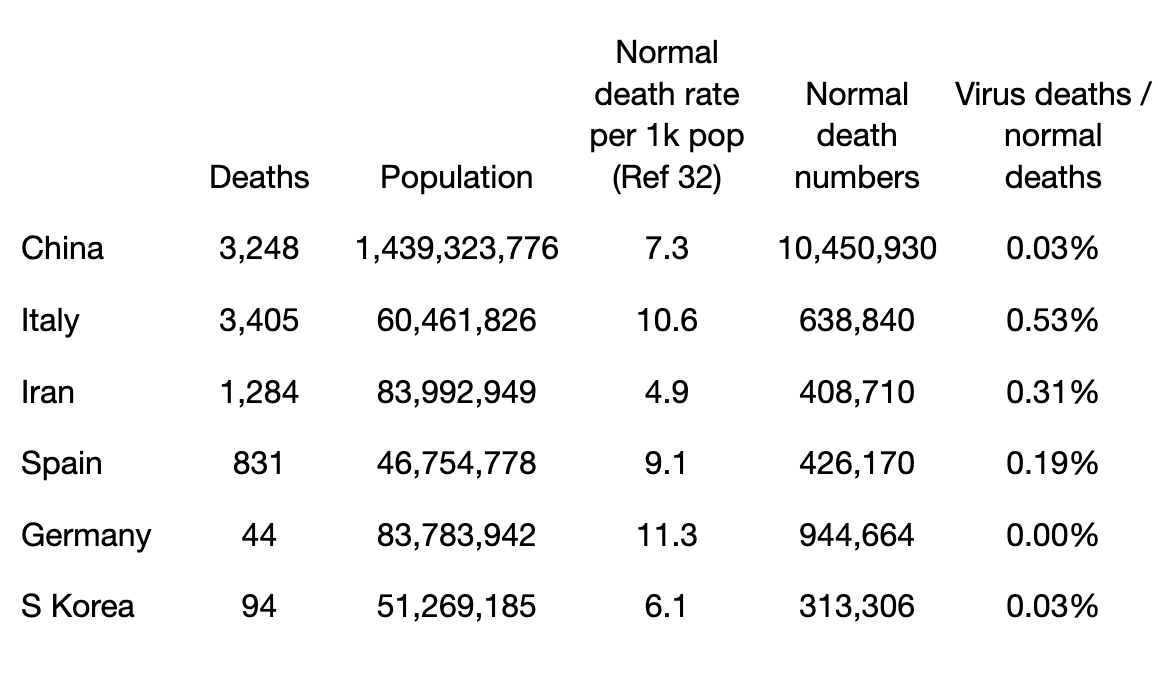
2) I have added a calculation into the table for the top five countries (plus S Korea) to put the number of deaths in perspective. Every death is a loved one lost. This is not to diminish the suffering that is being felt in any way. It is to provide perspective because perspective can ease fear and fear is as big an enemy as the virus right now:
3) Pollution kills an estimated seven million people worldwide each year. A number of deaths will have been avoided because economies have been operating far from normally (Ref 33).
Closing thought
Current deaths worldwide stand at 10,049. The flu claims approximately 400,000 lives every year, the majority of which – as with COVID-19 – are among the elderly and the vulnerable (Ref 34). We don’t close down nations and panic buy toilet rolls because of the flu.
There’s a lot of ‘scaring the life out of people’ going on right now – in print and online media and on social media. It isn’t helpful. Caution yes, catastrophising no. I hope that we will look back on this time and see that the above table was reflective of the outcome and COVID-19 barely made it onto the list of major causes of death for any country.
In the meantime, we need to be the best people we can be. The ones helping the vulnerable, not hoarding provisions for ourselves. I will always fear what humans can do to each other more than what any virus can do to ourselves.
References
Ref 1: https://www.who.int/health-topics/coronavirus and https://www.cdc.gov/coronavirus/types.html
Ref 2: Park et al. COVID‐19: Lessons from SARS and MERS. European Journal of Immunology. 27 Feb 2020. https://onlinelibrary.wiley.com/doi/10.1002/eji.202070035
Ref 3: https://www.nhs.uk/conditions/sars/
Ref 4: https://www.nhs.uk/conditions/middle-east-respiratory-syndrome-mers/
Ref 5: https://www.scmp.com/news/china/society/article/3074991/coronavirus-chinas-first-confirmed-covid-19-case-traced-back
Ref 6: Huang et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. January 24th 2020 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30183-5/fulltext
Ref 7: https://www.who.int/csr/sars/country/table2004_04_21/en/
Ref 8: https://www.who.int/emergencies/mers-cov/en/
Ref 9: https://www.cdc.gov/coronavirus/2019-ncov/cases-updates/cases-in-us.html
Ref 10: https://www.health.gov.au/news/information-about-the-first-confirmed-case-of-novel-coronavirus-in-australia
Ref 11: https://www.epicentro.iss.it/coronavirus/aggiornamenti
Ref 12: See 31st January update https://www.publichealth.hscni.net/news/covid-19-coronavirus
https://www.publichealth.hscni.net/sites/default/files/2020-02/COVID-19%20-%2031%20January%202020.pdf
Ref 13: The Sunday Times 15th March 2020. https://www.thetimes.co.uk/article/nadine-dorries-the-doctor-broke-the-news-i-had-the-coronavirus-and-i-gave-it-to-mum-hkx2hjpbd
Ref 14: http://www.pulsetoday.co.uk/views/blogs/as-a-gp-whos-overcome-coronavirus-heres-what-i-want-you-to-know/20040354.article
Ref 15: https://twitter.com/GoughCJ/status/1239587299136098305
Ref 16: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html
Ref 17: https://www.ncbi.nlm.nih.gov/pubmed/?term=covid+19
Ref 18: https://www.who.int/health-topics/coronavirus
Ref 19: https://www.cdc.gov/coronavirus/types.html
Ref 20: https://www.nhs.uk/conditions/coronavirus-covid-19/ and https://www.gov.uk/guidance/coronavirus-covid-19-information-for-the-public
Ref 21: https://www.health.gov.au/news/health-alerts/novel-coronavirus-2019-ncov-health-alert
Ref 22: https://www.worldometers.info/about/
Ref 23: https://experience.arcgis.com/experience/685d0ace521648f8a5beeeee1b9125cd
Ref 24: https://www.worldometers.info/coronavirus/
Ref 25: The top number (the numerator) will be accurate and the bottom number (the denominator) will be lower than it should be. This means that the rate – the top number divided by the bottom number – will be higher than the truth.
Ref 26: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19 — 16-march-2020
Ref 27: https://twitter.com/DavidVidecette/status/1238487118030258180
Ref 28: Parascandola & Xiao. Tobacco and the lung cancer epidemic in China. Transl Lung Cancer Res. 2019 May. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6546632/
Ref 29: https://www.weforum.org/agenda/2020/02/ageing-global-population/
Ref 30: https://www.thelocal.it/20200311/coronavirus-what-do-we-know-about-the-victims-in-italy
Ref 31: https://www.iss.it/en/comunicati-stampa/-/asset_publisher/fjTKmjJgSgdK/content/id/5304852
Ref 32: https://www.macrotrends.net/countries/CHN/china/death-rate (and then other countries can be searched)
Ref 33: https://www.who.int/health-topics/air-pollution#tab=tab_1
Ref 34: Paget et al. Global mortality associated with seasonal influenza epidemics: New burden estimates and predictors from the GLaMOR Project. J Glob Health. 2019 Dec. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6815659/
Get your copy from our Online Store or your local book and magazine retailer
Australian Retail Locations » Uncensored Publications Limited
New Zealand Retail Locations » Uncensored Publications Limited
As censorship heats up and free thought becomes an increasingly rare commodity, we appeal to our readers to support our efforts to reach people with information now being censored elsewhere. In the last few years, Uncensored has itself been censored, removed from the shelves of two of our biggest NZ retailers – Countdown Supermarkets and Whitcoulls Bookstores – accounting for 74% of our total NZ sales.
You can help keep the Free Press alive by subscribing and/or gifting a subscription to your friends and relatives.


Your information is a valuable contribution. Thank you.
Corona virus COVID-19- hype and hysteria? Demystification of the nightmare! https://youtu.be/JBB9bA-gXL4
Thanks Doreen
I do my utmost to keep a good balance and help with honest information in addition to the controversy that’s expected of Uncensored. Thanks for the Youtube clip.
Love to you
Martin